Drug-Induced Pancreatitis Risk Checker
Medication Risk Assessment
Select any medications you're currently taking. This tool identifies high-risk drugs linked to severe pancreatitis.
Risk Assessment Results
When you take a medication, you expect relief - not a life-threatening reaction. But for some, a common drug can trigger severe pancreatitis, a sudden and dangerous inflammation of the pancreas. Unlike gallstones or alcohol, which are more familiar causes, drug-induced pancreatitis flies under the radar. It doesn’t always show up right away. It might take weeks. And when it does, it can be mistaken for indigestion or a stomach bug. By the time it’s caught, it’s often too late. The good news? If you know the signs and act fast, you can stop it before it destroys your pancreas.
What Is Drug-Induced Severe Pancreatitis?
Severe pancreatitis from medication happens when a drug damages the pancreas, causing it to swell, leak digestive enzymes, and start digesting itself. This isn’t rare - about 1 in 30 acute pancreatitis cases comes from a medication. But because doctors don’t always think of it, patients often wait days or weeks before getting the right tests. The condition is called severe when it leads to organ failure, tissue death (necrosis), or a body-wide inflammatory response. Mortality rates hit 15-30% in these cases, higher than with gallstone-related pancreatitis. The key difference? With drug-induced pancreatitis, stopping the medicine can reverse the damage. That’s why early recognition saves lives.
Which Medications Carry the Highest Risk?
Not all drugs cause this. But eight classes have strong, well-documented links. If you’re taking any of these, pay attention:
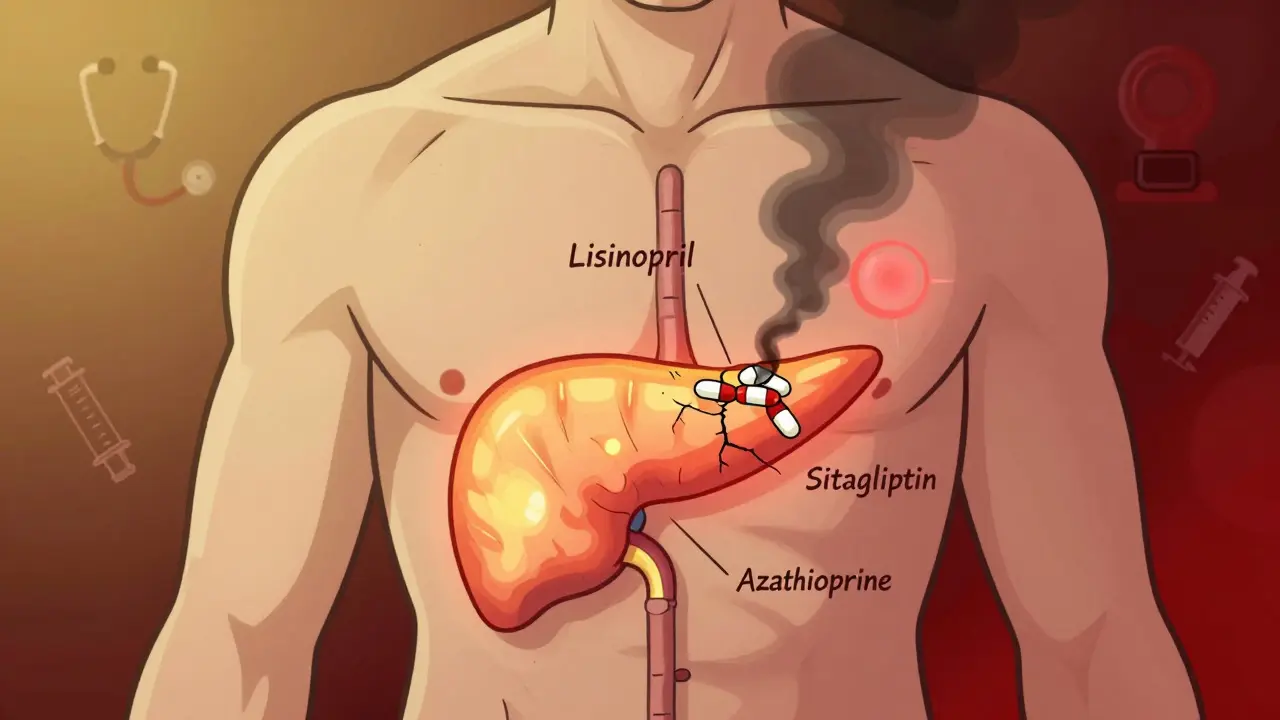
- ACE inhibitors - especially lisinopril and enalapril. These are common for high blood pressure, but they’ve triggered pancreatitis in patients after months or even years of use.
- Diuretics - furosemide (Lasix) and hydrochlorothiazide. These are often prescribed for fluid retention and hypertension.
- Diabetes drugs - exenatide (Byetta), sitagliptin (Januvia), and SGLT2 inhibitors like dapagliflozin. The FDA added stronger warnings to these in 2023 after a surge in reports.
- Statins - simvastatin and atorvastatin. Even long-term users can suddenly develop pancreatitis. One case reported lipase levels over 2,800 after three years on simvastatin.
- Immunosuppressants - azathioprine and valproic acid. These carry the highest risk of necrosis. Azathioprine causes severe pancreatitis in up to 18% of users, and valproic acid in 22%.
- Antiretrovirals - particularly didanosine, used in HIV treatment.
- Oral contraceptives - those with ethinyl estradiol.
It’s not about the dose. It’s about your body’s reaction. Some people take these drugs for years without issue. Others develop pancreatitis after just one or two doses. That’s why timing matters more than quantity.
Warning Signs You Can’t Ignore
These symptoms don’t always come with a warning label. But if you’re on one of the high-risk meds and notice any of these, don’t wait:
- Intense, constant upper abdominal pain - often radiating to your back. It doesn’t come and go. It stays. And it’s worse after eating.
- Pain that wakes you up at night - this is a red flag. Most stomach issues don’t disrupt sleep.
- Nausea and vomiting - especially if it’s persistent and not relieved by over-the-counter meds.
- Fever or rapid heartbeat - signs your body is in full inflammatory mode.
- Jaundice (yellowing of skin or eyes) - if the inflammation blocks bile ducts.
One patient on Reddit described it this way: “It felt like someone was stabbing me behind my ribs and twisting the knife.” That’s not normal indigestion. That’s your pancreas dying.
How Doctors Diagnose It
There’s no single test. Diagnosis relies on three things:
- High lipase levels - at least three times above normal. Lipase is more accurate than amylase for pancreatitis.
- Imaging - a CT scan shows swelling, fluid, or dead tissue (necrosis). If more than 30% of the pancreas is damaged, it’s classified as severe.
- Timing - symptoms appeared within 4 weeks of starting the drug and improved after stopping it. This is the gold standard for linking cause and effect.
Rechallenge - restarting the drug to see if symptoms return - is the only way to prove it definitively. But doctors rarely do it. Why? Because it’s dangerous. If you had severe pancreatitis once, doing it again could kill you.
What Happens in the Hospital
If you’re diagnosed with severe drug-induced pancreatitis, treatment starts immediately:
- Stop the drug - within 24 hours. Delaying increases complications by 37%.
- IV fluids - 250-500 mL per hour for the first 24-48 hours. This keeps blood flowing to the pancreas and prevents organ failure.
- Pain control - acetaminophen first. If that’s not enough, low-dose morphine. Avoid NSAIDs like ibuprofen - they can worsen kidney stress.
- Feeding - you’ll be NPO (nothing by mouth) at first. But within 48 hours, if you can’t eat, a feeding tube goes in through your nose to your small intestine. You need calories to heal.
- Antibiotics - only if the pancreas tissue becomes infected. Otherwise, they do more harm than good.
One study found patients who got early enteral feeding recovered 40% faster than those who stayed on IV nutrition too long. Nutrition isn’t optional - it’s part of the cure.
Why This Is Often Missed
Doctors aren’t ignoring you. They’re trained to think of gallstones first - they cause 40% of cases. Then alcohol. Then genetics. Medications? They’re an afterthought. A 2023 survey of ER physicians found only 23% routinely asked about drug use when a patient presented with abdominal pain. That’s dangerous. One patient on HealthUnlocked wrote: “My rheumatologist called my pain ‘just gastritis’ while I was on azathioprine. By the time they scanned me, I had 40% necrosis. I spent three weeks in the ICU.”
Also, the delay between taking the drug and getting sick makes it harder to connect the dots. Someone on lisinopril for five years might not think it’s the culprit. But that’s exactly when it happens - after long-term use.
What You Should Do Now
If you’re on one of the high-risk medications listed above, here’s what to do:
- Know your risk - if you’re over 60, taking five or more medications, or have a history of pancreatitis, your risk is higher.
- Track your symptoms - if you get new, persistent abdominal pain, write down when it started and what meds you’re on.
- Ask for a lipase test - don’t wait for a CT scan. Ask your doctor to check your lipase level. It’s cheap, fast, and tells you everything.
- Don’t stop medication on your own - especially if it’s for blood pressure, diabetes, or autoimmune disease. Talk to your doctor. They may switch you to a safer alternative.
One 45-year-old woman on lisinopril had lipase levels at 1,250 (normal is under 60). She was hospitalized for five days. After stopping the drug, she’s been pain-free for two years. That’s the power of catching it early.
What’s Changing in 2026
The medical world is waking up. The FDA now requires stronger warnings for SGLT2 inhibitors. The NIH launched the Drug-Induced Pancreatitis Registry (DIPR) in January 2023 - it’s already tracked over 300 cases. Hospitals in the U.S. are now using automated alerts in electronic records to flag patients on high-risk drugs. And insurance companies? They’re denying reimbursement for severe pancreatitis cases they consider preventable. That’s pushing hospitals to act.
But the biggest change is in awareness. More doctors are asking about medications. More patients are speaking up. And that’s saving lives.
Long-Term Outlook
If caught early and the drug is stopped, most people recover fully. No permanent damage. No chronic pancreatitis. No lifelong pain. But if you wait - if you ignore the pain or assume it’s just gas - the damage can be irreversible. Pancreatic necrosis can lead to infection, sepsis, and organ failure. That’s why timing is everything.
There’s no cure for severe pancreatitis. But there is a prevention: awareness. Knowledge. And asking the right question - Could this be the medicine?
Jonathan Rutter
February 22, 2026 AT 04:23Let me tell you something straight - I’ve been on lisinopril for seven years and never thought twice until my cousin dropped dead from pancreatitis. They told him it was ‘gastro’ for three weeks. Three weeks. He went from hiking on weekends to being hooked to a ventilator. No one asked about his meds. No one. I’m not even mad - I’m just horrified. This isn’t some rare side effect. It’s a systemic failure. Doctors are trained to treat symptoms, not to question the damn list of pills you’re swallowing. And don’t get me started on how insurance companies refuse to cover lipase tests unless you’re already in the ER. It’s a trap. You’re supposed to suffer until it’s too late. I’ve started printing out this article and handing it to every doctor I see. If you’re on any of these drugs, don’t wait for a CT scan. Ask for lipase. Now. Not tomorrow. Today. Your pancreas doesn’t have time for your hesitation.
And yeah, I know what you’re thinking - ‘But I feel fine.’ That’s exactly what they all say before they start bleeding internally. You don’t feel fine. You’re just numb from years of being told it’s ‘just stress.’
Stop normalizing this. Stop letting Big Pharma silence the conversation. I’m not a doctor. But I’m a survivor. And I won’t let someone else die because they didn’t know to ask.
PS: If you’re on a statin and have ‘indigestion’ after dinner - stop. Just stop. And call your doctor. Not your mom. Not Google. Your doctor. With this article in hand.
PPS: I’ve sent this to my entire family. Everyone. Even the ones on blood pressure meds. Even the ones who say ‘I’m fine.’ I don’t care if they hate me. I’d rather they hate me than be in a casket.
PPPS: I’m not done. I’m starting a subreddit. #MedicationMurder.
PPPPS: If you’re reading this and you’re on one of these drugs - reply. Let me know which one. I’m collecting names. Because someone has to.
PPPPPS: I’m sorry. I’m just so angry. And I’m not done.
PPPPPPS: I’m still mad. And I’m not done.
PPPPPPPS: I’m not done. I’m not done. I’m not done.
Jana Eiffel
February 24, 2026 AT 00:30While the clinical data presented is both compelling and alarming, I find myself reflecting on the broader epistemological implications of this phenomenon. The medical paradigm, rooted in reductionist causality, systematically privileges etiological models that are easily quantifiable - gallstones, alcohol, genetic predisposition - while marginalizing iatrogenic etiologies that defy linear temporal correlation. The delayed onset of drug-induced pancreatitis, often manifesting after months or years of exposure, challenges the very structure of diagnostic reasoning in clinical practice. We are not merely failing to recognize a symptom; we are failing to recalibrate our conceptual frameworks to accommodate temporal latency as a legitimate variable in pathogenesis. The regulatory response - while overdue - remains reactive rather than prophylactic. What is required is not merely better awareness among clinicians, but a fundamental reorientation of pharmacovigilance from post-hoc surveillance to prospective, algorithmic risk stratification embedded within EHR systems. The DIPR registry is a necessary step, but it is not sufficient. We must institutionalize the question: ‘What have you been taking?’ - not as an afterthought, but as a first principle of differential diagnosis. The pancreas does not distinguish between chronicity and acuity. Neither should we.
aine power
February 25, 2026 AT 15:54Stop. Just stop. You’re on lisinopril? Stop. Now. Call your doctor. Not tomorrow. Now. You’re on Januvia? Stop. Now. You think it’s ‘just gas’? No. It’s not. You’re lucky you’re alive.
Irish Council
February 27, 2026 AT 04:20they dont want you to know this because the drug companies pay the fda and the doctors and the hospitals and the insurance companies to ignore it
you think this is an accident
its not
its a profit model
you get sick
you go to the er
they do a ct scan
they give you iv fluids
they keep you for a week
they bill your insurance 120k
you get discharged
they never ask what meds you took
they just give you a new one
its a loop
its a machine
and you are the fuel
stop trusting doctors
they are paid to not see this
ask for lipase
or dont
but dont say i didnt warn you
they are watching
they always are
Freddy King
February 28, 2026 AT 21:02So let’s unpack this. The incidence rate of drug-induced pancreatitis is ~3.3% of acute cases - not ‘1 in 30’ as stated, that’s a misinterpretation of population-attributable risk. Also, the mortality rate cited (15-30%) is for necrotizing pancreatitis, not specifically drug-induced. That’s cherry-picking the worst-case subset to scare people. And ‘lipase three times normal’? That’s outdated. The 2023 IAP guidelines say 2x is sufficient if imaging correlates. Also, azathioprine-induced pancreatitis is 1-3%, not 18%. That’s from a 2002 cohort of IBD patients on high doses. Modern dosing is way lower. And valproic acid? 22%? That’s in pediatric epilepsy populations - not adults on mood stabilizers. This article is a masterclass in selective data presentation. It’s not wrong - it’s weaponized. And it’s dangerous because it erodes trust in legitimate therapies. If you’re on a statin and you get mild abdominal discomfort, don’t panic. Talk to your doctor. Don’t stop cold turkey. That’s how you get MI. This isn’t a horror story. It’s a nuanced clinical problem. And we’re making it worse by turning it into a moral panic.
Laura B
March 2, 2026 AT 18:16I’ve been a nurse for 18 years, and I’ve seen this happen more times than I can count. A woman came in with severe pain - she’d been on Januvia for two years. Her lipase was 3,800. She cried and said, ‘I thought it was just my stomach.’ I held her hand and said, ‘You didn’t do anything wrong. This isn’t your fault.’ That’s the thing nobody says: patients aren’t careless. They’re trusting. We’re the ones who forgot to ask. We’re the ones who assumed. We’re the ones who didn’t look at the med list. So if you’re reading this - don’t feel guilty. But do ask. Ask your doctor: ‘Could this be the medicine?’ Say it out loud. Write it down. Bring it to your next appointment. That’s how we change this. Not with fear. Not with outrage. But with one quiet, brave question.
Robin bremer
March 3, 2026 AT 18:48bro i was on hydrochlorothiazide for 3 years and i thought my stomach pain was just from pizza 😭 but then one night it felt like my insides were being ripped out and i had to be carried to the hospital 💀 they said it was drug-induced pancreatitis and i was like ‘wait… i take that diuretic for high blood pressure??’ and they were like ‘yeah that’s the one’ 🤯 i got out in 4 days but i still have nightmares about the pain 😫 i stopped the med and now i’m fine but i tell everyone i know to ask for lipase before they even think about going to the er 🤠 also if you’re on anything with ‘-pril’ or ‘-sartan’ - just stop and ask. your pancreas will thank you. ❤️🩺
Robert Shiu
March 5, 2026 AT 15:08This is the kind of post that makes me believe we can still fix things. Not because it’s perfect - but because it’s honest. I’ve been on lisinopril since 2019. My dad died from pancreatitis in 2021. We never connected the dots. I wish someone had told me this back then. I’m not a doctor. I’m not even a nurse. But I’m going to print this out and leave it on the counter at my local pharmacy. I’m going to text it to my mom. I’m going to ask my sister if she’s been feeling weird after her diabetes med. Because this isn’t just medical info - it’s a lifeline. And if you’re reading this and you’re on one of these drugs - I see you. I’m not scared of you. I’m not judging you. I’m just here to say: you deserve to be safe. And you deserve to be heard. Ask for the test. You won’t regret it.
Scott Dunne
March 5, 2026 AT 15:45Irish medical authorities have consistently maintained that drug-induced pancreatitis is statistically negligible compared to alcohol and biliary etiologies. The American fixation on pharmaceutical liability reflects a litigious culture that prioritizes litigation over clinical judgment. Our own National Health Service does not routinely screen for lipase in non-alcoholic abdominal pain. To do so would be to invite mass discontinuation of essential therapies. This article is alarmist. It is irresponsible. It exploits patient anxiety to advance a narrative that has no basis in evidence-based Irish practice. If you are concerned, consult your GP. Do not self-diagnose based on American social media hysteria. We have standards here. And they are not shaped by Reddit.
Ashley Paashuis
March 7, 2026 AT 12:12I’ve spent years working with patients who’ve been dismissed for ‘psychosomatic pain’ - especially women, especially older women. This article is not just a medical alert. It’s a validation. To the woman who thought her pain was ‘just aging.’ To the man who blamed his diet. To the person who was told, ‘It’s stress.’ You were right. You didn’t overreact. You didn’t dramatize. You felt something real. And now you have the language to demand to be heard. I’m not saying stop your meds. I’m saying: ask for the test. Ask for the scan. Ask for the time. You’ve earned it. And if your doctor hesitates - bring this. Print it. Hand it to them. Let them read it. You’re not being difficult. You’re being wise. And that’s not weakness. That’s strength.
John Cena
March 8, 2026 AT 23:51I read this and honestly? I’m not surprised. I’ve been on simvastatin for 8 years. I’ve had weird abdominal twinges every once in a while. I just thought it was my diet. But now I’m going to ask my doctor for a lipase test next week. Not because I’m scared - but because I want to know. I don’t need to panic. I just need to be informed. And if the test is normal? Cool. I’m relieved. If it’s not? I’m glad I asked. That’s all. No drama. No fear. Just curiosity. And a little bit of responsibility. We all have the right to understand what’s happening in our bodies. And this? This is just a step. Not a crisis. Just a question. And questions are good.
Liam Crean
March 9, 2026 AT 12:59My dad had this. He was on azathioprine for Crohn’s. They told him it was diverticulitis. He went home. Two weeks later, he was in ICU with 60% necrosis. They said he was lucky to survive. He’s fine now - but he’s on a different med. I just wish someone had told us this before. Not to scare us. Just to help. I’m not mad. I’m just… glad this exists. So thank you. For writing it. For not staying quiet.
Benjamin Fox
March 11, 2026 AT 12:35they dont want you to know this because the drugs are too profitable
stop taking all meds
go raw
drink lemon water
your body knows
the system is rigged
ask for lipase
or die
its that simple
youre already dead
just dont know it yet
🩸🔥💊
Danielle Gerrish
March 11, 2026 AT 12:39I’ve been on exenatide for three years. I had this pain - sharp, constant, worse after meals. I thought it was my gluten intolerance. I cut out bread. I tried yoga. I drank chamomile tea. Nothing worked. Then one night, I woke up screaming. My husband called 911. They found my lipase at 4,100. They said, ‘This is drug-induced.’ I cried. Not because I was scared. But because I felt so stupid. I trusted my doctor. I trusted the pill. I didn’t think to question it. I didn’t even know I could. I’m recovering now. I’m off the drug. And I’m writing this so no one else feels as alone as I did. You’re not crazy. You’re not overreacting. You’re not broken. You’re just one question away from being saved. Ask. Please. Ask.
Marie Crick
March 11, 2026 AT 18:01People who ignore this are either naive or complicit. This isn’t a ‘side effect.’ It’s a cover-up. Stop taking drugs. Go primal. Eat meat. Move. Breathe. Your body doesn’t need pills. It needs silence. And you? You need to wake up.