Hyponatremia management: what to do first and how to stay safe
Low sodium (hyponatremia) is common and can be harmless or life-threatening. The tricky part is that fixing sodium too fast can cause serious brain injury. So the goal is clear: find the cause quickly, treat the problem safely, and monitor sodium closely.
Quick assessment steps
Start by checking how the patient looks and how fast the sodium dropped. Symptoms range from mild (nausea, headache, tiredness) to severe (confusion, seizures, coma). Acute drops (under 48 hours) are more dangerous than chronic drops. Lab tests that help: serum sodium and osmolality, urine osmolality and urine sodium, and a basic volume check—are they low on fluid (hypovolemic), normal volume (euvolemic), or overloaded (hypervolemic)?
Also review medicines: common culprits include thiazide diuretics, some antidepressants (SSRIs), anticonvulsants, and certain pain drugs. Check for heart failure, liver disease, kidney problems, recent surgery, or heavy drinking—these often point to the cause.
Treatment options and safety rules
Mild, chronic cases often do well with simple measures: stop the offending drug, limit free water (typical target 800–1,000 mL/day for SIADH), and treat the underlying illness. For hypervolemic hyponatremia from heart failure or cirrhosis, fluid and sodium restriction plus loop diuretics are common approaches.
When sodium is low enough to cause serious symptoms, hospital care is needed. Doctors may use controlled hypertonic saline (3%) under close monitoring. The key safety rule: avoid raising serum sodium too fast. Most guidelines recommend not increasing sodium by more than 8 mmol/L in 24 hours; in high-risk patients (very low sodium, malnutrition, alcoholism) aim for 4–6 mmol/L per 24 hours. Check sodium every 2–4 hours while correcting.
For stubborn or chronic SIADH, options include oral salt plus loop diuretics, demeclocycline, or vasopressin receptor antagonists (vaptans). Vaptans work well but need specialist oversight, liver checks, and careful monitoring because they can correct sodium quickly.
Always tailor treatment to cause and risk. A patient with mild, stable hyponatremia can often be managed outpatient with clear follow-up. Any patient with seizures, severe confusion, coma, or very low sodium needs urgent hospital assessment.
If you or someone you care for shows worrying symptoms—sudden confusion, severe headache, repeated vomiting, or a seizure—get emergency help. Proper testing and careful correction make the difference between a safe recovery and serious complications.
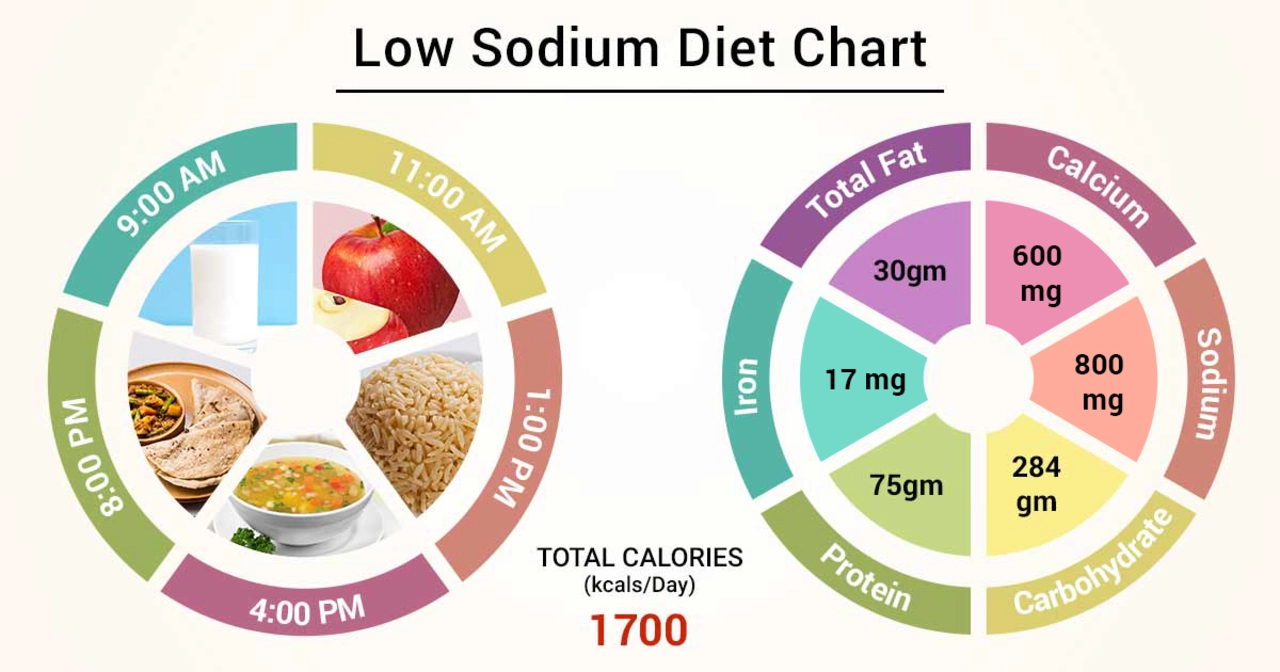
The Role of Diet in Preventing and Managing Hyponatremia
- by Colin Edward Egan
- on 15 May 2023
In my latest blog post, I discussed the role of diet in preventing and managing hyponatremia, a condition characterized by low sodium levels in the blood. I emphasized the importance of maintaining a balanced diet, which includes consuming adequate amounts of sodium to help regulate fluid balance in the body. In addition, I explored how drinking enough water, avoiding excessive consumption of sodium-rich foods, and being mindful of medications can help prevent and manage this condition. By paying attention to our diet, we can greatly reduce our risk of developing hyponatremia and lead a healthier life. Stay tuned for more tips on maintaining a balanced diet and overall well-being!