PDE5 Inhibitor Safety Window Calculator
Use this tool to determine if enough time has passed since your last dose of a PDE5 inhibitor to safely use nitrates (like Nitroglycerin). Disclaimer: This is for educational purposes; always follow your doctor's specific prescriptions.
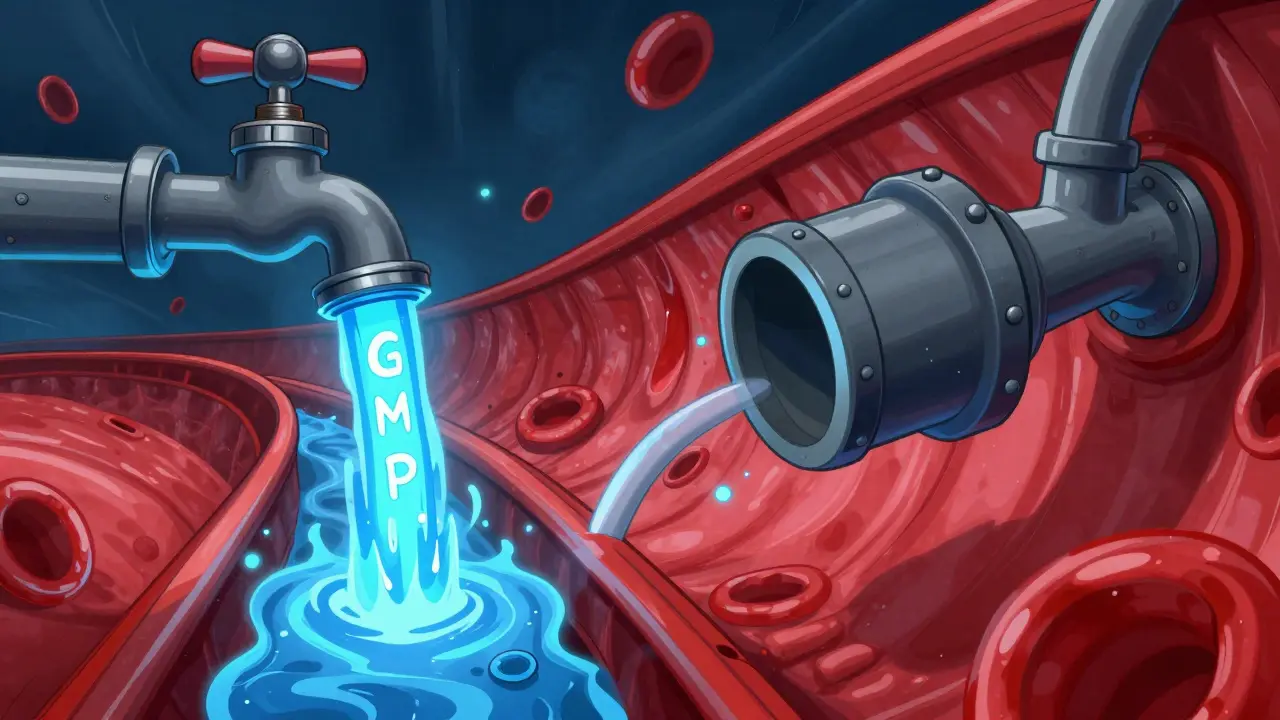
The Molecular Collision: How cGMP Overload Happens
To understand the profound hypotension mechanism, you have to look at the cGMP pathway as a faucet and a drain. Nitrates are like turning the faucet on full blast, flooding the vascular smooth muscle cells with cGMP. Normally, the PDE5 enzyme acts as the drain, letting the cGMP out so the blood vessels can regain their tone and maintain a steady blood pressure. When a person takes a PDE5 inhibitor, they effectively plug that drain. If you turn the faucet on (nitrates) and plug the drain (PDE5 inhibitors) at the same time, cGMP accumulates to extreme levels. This surplus of cGMP activates protein kinase G, which forces calcium out of the cell's cytoplasm. Since smooth muscles need calcium to contract, the loss of calcium means the muscles stay permanently relaxed. This isn't just a local effect; it's systemic. Every blood vessel in the body begins to widen simultaneously. This massive, widespread vasodilation leads to a sudden drop in systemic vascular resistance. In a clinical setting, this can manifest as a systolic blood pressure (SBP) plummeting below 85 mm Hg. For some patients, this results in immediate fainting, shock, or even cardiac arrest because the heart cannot pump enough pressure to reach the brain.Timing the Danger: Half-Lives and Safety Windows
Not all PDE5 inhibitors are created equal when it comes to how long they stick around in your system. This is why the "waiting period" differs depending on which pill you took. The risk persists as long as the inhibitor is active enough to block the PDE5 enzyme.| Medication | Approximate Half-Life | Required Gap Before Nitrates |
|---|---|---|
| Sildenafil (Viagra) | 4 hours | 24 hours |
| Vardenafil (Levitra) | 4 hours | 24 hours |
| Avanafil (Stendra) | 5-6 hours | 24 hours |
| Tadalafil (Cialis) | 17.5 hours | 48 hours |
The Real-World Debate: Theory vs. Practice
For decades, the medical community has treated the combination of nitrates and PDE5 inhibitors as an absolute contraindication-meaning you simply never do it. However, recent data has sparked a bit of a debate among cardiologists. A large US-based study analyzing electronic health records found that thousands of patients were co-prescribed these drugs without experiencing a significant increase in heart attacks or blood pressure crashes. Why the discrepancy? It's likely because patients in the real world are better at self-managing. Someone might skip their long-acting nitrate on a day they plan to use a PDE5 inhibitor, or they may naturally space them out. Furthermore, some evidence suggests that PDE5 inhibitors might actually help the heart by improving endothelial function. Despite this, the American Heart Association and the FDA maintain the strict warning. The logic is simple: while the *likelihood* of a crash might be lower than the chemistry suggests, the *severity* of a crash is too high to gamble with. A single instance of profound hypotension can be fatal, making the risk-benefit ratio lean heavily toward avoidance.Emergency Protocols: What to Do During a Crash
If a patient accidentally takes both medications and begins to feel dizzy, faint, or breathless, every second counts. The goal is to get blood back to the brain and heart immediately.- Immediate Positioning: Place the person in the Trendelenburg position. This means laying them flat on their back and elevating the feet above the level of the heart. This uses gravity to push blood from the legs back toward the core.
- Emergency Contact: Call emergency services immediately. It is vital to tell the paramedics exactly which PDE5 inhibitor was taken and when, as well as the type of nitrate used.
- Medical Intervention: In a hospital setting, doctors will use intravenous (IV) fluid resuscitation. By pumping fluids into the veins, they increase the "preload" (the volume of blood returning to the heart), which helps raise the blood pressure back to a safe level.

Navigating the Dilemma for Heart Patients
If you are a man with stable coronary artery disease who also struggles with ED, you don't have to simply give up on one of the treatments. There are safer paths to management. The Princeton IV consensus suggests that doctors should first re-evaluate whether nitrates are absolutely necessary. Since coital angina (chest pain specifically during sex) only affects about 15-20% of men with heart disease, many patients can be switched to alternative anti-anginal medications.Consider switching to Beta-blockers or Calcium Channel Blockers. These drugs manage heart rate and blood pressure without donating nitric oxide, meaning they don't trigger the cGMP accumulation cascade. This allows a patient to safely use a PDE5 inhibitor for ED while still protecting their heart.
Final Safety Checklist
To avoid a dangerous interaction, keep these rules of thumb in mind:- Check the clock: Wait 24 hours for Sildenafil/Vardenafil/Avanafil and 48 hours for Tadalafil before using any nitrate.
- Avoid 'Poppers': Never use recreational nitrites if you have taken a PDE5 inhibitor in the last few days.
- Communicate: Ensure every doctor you see knows about both your heart medications and your ED prescriptions.
- Carry a Warning: Use a wallet card that lists your medications and the required waiting periods for emergency responders.
Can I eat foods high in nitrates, like spinach or beets, while taking Viagra?
Yes. Dietary nitrates and L-arginine supplements do not provide enough plasma nitric oxide to trigger the dangerous cGMP accumulation associated with pharmaceutical nitrates. They are generally safe and do not cause profound hypotension.
Is nitrous oxide (laughing gas) safe with PDE5 inhibitors?
Generally, yes. Nitrous oxide anesthesia used in dental or medical procedures does not produce the same pharmacological effect as organic nitrates like nitroglycerin and does not typically result in clinically significant hypotension when combined with PDE5 inhibitors.
What are the symptoms of the interaction between these drugs?
The primary symptom is a sudden, severe drop in blood pressure. This feels like extreme dizziness, lightheadedness, a racing heart (tachycardia) as the body tries to compensate, blurred vision, and potentially fainting or loss of consciousness.
Why does Tadalafil require a longer waiting period than Sildenafil?
Tadalafil has a much longer half-life (about 17.5 hours) compared to Sildenafil (about 4 hours). Because it stays in your blood and continues to block the PDE5 enzyme for much longer, you need a 48-hour gap to ensure the drug has cleared your system enough to avoid a crash.
Can a doctor ever prescribe both medications to the same patient?
While officially contraindicated, some specialists may allow conditional use in highly selected, stable patients with strict timing protocols. However, this is considered off-label and requires intense patient education and supervision. For most people, the standard is total avoidance.